I mean, yeah, current implants are shit. They might be shit for the next 100 years. Medicine was shit for a good time, too. So while right now the best implants provide is the novelty factor, I think we'll eventually see them as just another normal thing. See this article, for example, where they might have created a sensor that is actually harmless and dissolves. You just need the right materials. Your reddit post's example with obsolescence is a good one, but we can also overcome that (theoretically), via stuff like nanobots that can dismantle/upgrade implants in a less invasive way, for example.
And we might not even need that open wound for a 'jack in the future - Just look at how wireless technology has improved over the last decade.
Oh, also that guy with the camera is colourblind. Which is why he has that camera.
There's only one version of Moore's law that is true in biology. Sequencing:

Past that, most of medicine follows linear progress or sudden breakthrough.
You'd have better luck listening to Drew Endy expound on reprogramming cells through synthetic biology than OP's guys talk about sticking home-made electronics under their skin. And even there...

Plateaus, not skyrockets.
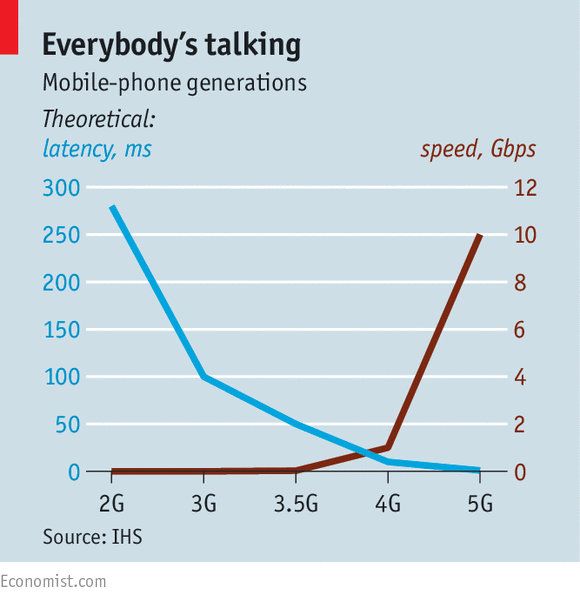
I was talking about wireless transmission making wires unnecessary, which means we don't need to break the skin. Today's bandwidth isn't good enough, but that in five years might be enough for, I dunno, real-time single-cell recordings or somesuch.
You're still talking about putting done device under the skin. Wires out or no. Pretty much every organ of your body has immune cells that will be on the lookout for a metal / coated coated object.
For example, single cell neuronal recordings are done with electrodes that pick up on the induced electrical field of those cells firing. No breaking of cell membranes involved. But they are still notorious for losing signal after a month (in mice) as the glial cells in the brain form a scar around the device.
I mean, yeah, implants will always be shit.
This is a discussion I have whenever implants come up, because people such as yourself think that Moore's Law applies to immunology. It doesn't. Until we genetically engineer humans to specifically not reject a specific selection of foreign materials, humans will continue to reject all foreign bodies. The way around it, which I worked on back when I thought I wanted to do this shit for a living, is to engineer nanostructures small enough that the body doesn't attack them... but since the body attacks, you know, viruses, you start working with structures about the size of asbestos fibers which, by the way, are carcinogenic. Or, you know, you CRISPR up your babies so that they think titanium is a part of their bodies and then within ten years you've got viruses and bacteria that imitate titanium.
That's the other part of the problem: because any implant site is a wound, any implant site is subject to opportunistic infection and everything else has a much faster evolutionary cycle. I can't remember the exact numbers, but the number of generations humans have experienced since Australopithecus is the same as drosophila have experienced since the 1930s, and e.coli have experienced since two weeks ago. Being long-lived means you have a lot of genetic inertia, for better and worse.
The "right" materials, as you outline them, are materials that go away. Did you miss that?
- Here, we report materials, device architectures, integration strategies, and in vivo demonstrations in rats of implantable, multifunctional silicon sensors for the brain, for which all of the constituent materials naturally resorb via hydrolysis and/or metabolic action, eliminating the need for extraction.
They're dealing with the very problem I describe: leave the implant in and it will kill or maim the patient. Your answer? Grey goo.

Theoretically, nanomachines can turn my stale coffee into diamonds. Practically, a nanomachine is a tiny, rudimentary thing that requires preposterous amounts of support infrastructure to do something really simple in miniature. A future in which that sort of omnipotent nanotechnology exists is one that belies implants entirely: why should I worry about an interface jack that doesn't rot when I can just have the magic grey goo restructure my brain while I wait?
I get that the guy is colourblind. My point is that there's no aspect of a singing camera that needs to be surgically attached to your body. That's an iPhone app, yo.
No part of that needs to be surgically stitched to you. My suspicion is that he decided to be hipsterish about it and spike a transducer into his skill so he got it via bone conduction but fuckadoodle doo. My library sells earbuds for a buck a piece. The reasons for not stitching that shit into your skull are legion.
Also lesion.
I'll show myself out.
Obiously if you had nanotech you wouldn't go for a fucking chrome arm. It does deal with the problem of surgeries and the open wound thing, and how old implants may become out-of-date pretty fast. It replaces a surgical procedure with something more akin to upgrading your smartphone.
The interesting point about the brain sensor article wasn't the melting away - it was that there was no immunoresponse. It'd probably happen if you waited a bit longer, but we do have materials that don't inflame immediately. Which shows that there's still progress to be made.
I'm also surprised that you claim "any implant site is subject to opportunistic infection and everything else has a much faster evolutionary cycle.". What about hip implants? That's a fairly huge metal thing in your thigh. What about cochlear implants? (Or breast implants) They stay in your body, sometimes for your whole life.
Saying that we do not have useful implants is just plain wrong, we do, and they are routinely used. And they improve people's lives. They might not make people better at something they did before (except maybe breast implants?), but I doubt it's gonna stay that way for long. In fact, runners with prosthetic legs can already be faster than normal runners (which is just a narrow employ of legs, though, so in my opinion that doesn't count).
We can avoid the immune response on two ways: Suppressing the immune system, which is probably a bad idea.
The other idea is, of course, to avoid drawing the immune system's response altogether. And we can already do that, by coating it with biocompatible materials like collagen or PEG. The problem is to keep the body from reacting with the implant itself.
Point by point:
- The interesting point about the brain sensor article wasn't the melting away - it was that there was no immunoresponse.
Right. Like catgut or nylon sutures. There's no immunoresponse there because the irritant goes away. So yeah - if you want to put in an implant that is only going to last a couple weeks, hip hip hooray.
- I'm also surprised that you claim "any implant site is subject to opportunistic infection and everything else has a much faster evolutionary cycle.". What about hip implants?
They have a design life of about 20 years. My grandfather went through two. Atrial cardioverters? 10 years. Ventricular cardioverters? 6-8 years. That's the calculus: "Will you be dead by the time this thing fails?" Cochlear implants? Dunno, not my bag... but not as long as you. Breast implants? I've known women who had to get them redone under warranty (typically 10 years); apparently every year, between 1% and 3% of all boob jobs are getting redone.
And these are simple, mechanical things. A saline sack or a titanium jack are doing a lot less than, say, bluetooth.
- Saying that we do not have useful implants is just plain wrong, we do, and they are routinely used.
Good thing I didn't say that. What I said was "There are no implants of any kind, nor will there ever be, that will leave you better off than if you didn't have them because your body doesn't like having non-body stuff in it." To be even clearer, I said "Ain't nobody gonna begrudge a blind man an electric eye." And so that we're absolutely lucid, that blind man would much rather have your eyes than a 256-pixel light-dark grid, but he'd rather have the grid than nothing.
- They might not make people better at something they did before (except maybe breast implants?), but I doubt it's gonna stay that way for long.
That is because you are uneducated in this subject, and are confusing "wish" with "understand."
- In fact, runners with prosthetic legs can already be faster than normal runners (which is just a narrow employ of legs, though, so in my opinion that doesn't count).
Sure - but if I attach Pistorius' springboard to my shoes, I can run faster than Pistorius. Besides which, that's a prosthetic, not an implant. Reductio ad absurdum on that is that a forklift is a prosthetic lifter.
- The other idea is, of course, to avoid drawing the immune system's response altogether. And we can already do that, by coating it with biocompatible materials like collagen or PEG.
Wishing doesn't make it so.
- So yeah - if you want to put in an implant that is only going to last a couple weeks, hip hip hooray.
Eh, if we're talking implanting stupid shit into yourself, most people might be satisfied with it lasting only a few weeks.
- They have a design life of about 20 years. My grandfather went through two. Atrial cardioverters? 10 years. Ventricular cardioverters? 6-8 years. That's the calculus: "Will you be dead by the time this thing fails?"
Hip replacements don't fail because the immune system kills them, though. They're worse at wear and tear than original bones. Pacemakers have to be swapped because battery. Nothing to do with their compatibility. For pacemakers, the original leads might stay in forever.
- And these are simple, mechanical things. A saline sack or a titanium jack are doing a lot less than, say, bluetooth.
Bluetooth is a bad example because that's just as non-interactive as the others. A memory brain implant that connects to actual nerves, maybe. Bluetooth would just be another box.
- And so that we're absolutely lucid, that blind man would much rather have your eyes than a 256-pixel light-dark grid, but he'd rather have the grid than nothing.
Yeah, but I'm saying that progress is inevitable, and if we can have a 256-pixel grid, we can get up to and beyond original eyesight.
- Wishing doesn't make it so.
Nothing to do with wishing, it already works. Example.
- Hip replacements don't fail because the immune system kills them, though. They're worse at wear and tear than original bones.
This is simply not true. My grandfather's implant, for example, was in splendid shape... but the bone around it had impacted and eroded so fiercely that one leg was 3/4" shorter than the other.
- Pacemakers have to be swapped because battery. Nothing to do with their compatibility. For pacemakers, the original leads might stay in forever.
This is also simply not true - you're speaking to someone who spent a year designing and testing implantable shock/pace leads for atrial defibrillators. The implantation helices lose conductivity due to plaque build-up and the conduction coils wear mechanically. Again, our design life was ten years. I built the testers to simulate ten years of normal wear on implantable shock/pace leads. And I broke them.
- Yeah, but I'm saying that progress is inevitable, and if we can have a 256-pixel grid, we can get up to and beyond original eyesight.
Yeah, but I'm saying you're wrong. The progress you're looking for is on the body side, not on the gadget side, and in case you hadn't noticed, that side is not progressive.
- Nothing to do with wishing, it already works. Example.

- but the bone around it had impacted and eroded so fiercely that one leg was 3/4" shorter than the other.
Which, again, nothing to do with the implant being rejected. The bones being eroded by the metal why we have metal-on-metal hip replacements now.
- I built the testers to simulate ten years of normal wear on implantable shock/pace leads. And I broke them.
Cool, how do you test that?
The link to the paper works for me. It's basically about how a coat makes a titanium rod bond better with bone (helping it heal fast). So, very much a thing:
- "All implants healed uneventfully without wound infection, implant loosening or chronic adverse reaction during the whole course of the experiment. In particular, no abundant lymphocyte or granuloclyte infiltration and no appearance of multinucleated giant cells (apart from osteoclasts) has been observed at any time."
Even after 28 days, no reaction.
- that side is not progressive.
Bacteria becoming resistent to antibiotics faster than we create them has nothing to do with developing materials that don't trigger the immune system.
You seem to think that we will never be able to develop something that makes our bodies accept implants. Apparently, the immune system is so great at sniffing out foreign substances that we will never be able to trick it. Never is a very bold claim to make. One that isn't supported by the evidence.
Moving the goalposts again, and also being factually wrong. Do you remember why my grandfather's hip came into the discussion?
- Hip replacements don't fail because the immune system kills them, though. They're worse at wear and tear than original bones.
They're not. They're titanium. they're strong as fuck. But let's roll right into the riposte:
- Which, again, nothing to do with the implant being rejected. The bones being eroded by the metal why we have metal-on-metal hip replacements now.
WE'RE NOT METAL. At some point, the implant has to touch gooey meaty bits. Or crunchy chalky boney bits. Generally both, if you're talking a hip replacement as that shit goes into marrow. So let's review:
- Leg without titanium: shortened normally
- Leg with titanium: accelerated decrepitude
- difference: Titanium
It's pretty simple math but you keep dancing around it by pretending you don't understand. Like the paper you linked to that I can't get to that says "holy shit, no reaction in four weeks." Dude, I got milk that lasts longer than that. If your implant expires faster than dairy products it isn't applicable to the subject of transhumanism. Nobody says "I want awesome cyber shit in my body for the next couple weeks" they say "I wanna be awesomely cyber." You're essentially arguing the temporary tattoos of implantation and extrapolating out to permanence. And I'm not willing to assume you're doing it by accident.
Like your canard about bacterial resistance. Once more, with feeling: an implant site is a wound, its success is directly correlated with immune response, and subverted immune response is a pathway to infection. Full stop.
Our bodies will never accept implants. I've done the vivisection. I've reviewed the studies. I've been involved in the primary research. You're still going for this "fundamental advancement of medical technology" thing and ignoring the fact that human immune systems are unchanged from the time of Solomon.
And the worst part is you pretend you don't even understand the evidence. Here, watch:
_________________________________________________________________________
- Cool, how do you test that?
The primary failure modes for implanted shock/pace leads are related to body motion. Because the most likely site for a cardioverter is underneath the pectoralis via Superior Vena Cave (SVC) cutdown with cardiac access through the svc, leads generally travel up underneath the clavicle and back down. Rotator action (swinging the arm, either while walking or with a tennis racket, for example) provides compression upon the lead. Generalized motion causes the attitude between cardioverter and fixation site to change by a small but non-negligible amount.
The FDA will sign off on any test they feel adequately reflects the failure mode of your product. In our case, our leads were made of helical small-gage MP35N, a cobalt-nickel alloy with high corrosion resistance and excellent conductivity. The coil was sheathed in implantation-grade medical tubing the composition and coatings of which were not my job; existing tests proved that their eventual breakdown by the body did not have substantially adverse effect on the charge delivered to the heart. Therefore, our primary concern was physical breakage of the coil.
The first test, flexion, consisted of counter-rotating chucks each containing the end of a sample of our coil. I designed, built, tested and deployed a 3/4 HP test rig that spun 24 of these 4" samples at 10,000 RPM, like an Epilady from hell:

Each rotation of the sample passed it through a complete 180 degree bend and back, without the cooling or hysteresis period that the actual lead would experience within the body. Also, atrial fibrillation patients aren't really in the habit of doing anything at 10,000 RPM so the conditions experienced by the leads were worst case, to say the least. As it is, our leads could survive approximately 18 hours of destructive testing at 10,000 RPM.
Assume your patient will live 20 years. If the leads in his body somehow go through a complete 180 degree bend and back again 1500 times a day, he might need a replacement. Otherwise, he's probably good.
The other test involved compression in a medium that modeled tissue. I developed a roller system and poured samples of a medical moulding compound that rolled the leads over and over again until they broke down. The tricky part was finding a molding compound that would survive long enough to cause the coils to deform. As it turns out, cobalt-nickel alloy is pretty tough.
BUT NONE OF THAT SHIT MATTERED because the scar tissue that built up at the helix site rendered the leads moot after about ten years. Less, if the patient was particularly unhealthy (none of our patients were particularly healthy, much like every other implant candidate in the history of medicine). And the body could break down the sheathing and plaque up the inside of the helix and it didn't matter because it was bioinert... but the simple presence of the lead caused a substantial portion of the body's immune defenses to be redirected towards plaqueing the lead over. After five years in a sheep, what was a 1/6" diameter pace lead ended up looking like linguini.
________________________________________________________________________________________
The shit you build? Solid as fuck. That flexion tester sounded like a goddamn lear jet (I kinda fucked up the gear lash - what can I say, I was an undergrad). The body you put it in? Frail, and made out of meat.
You can't fix the meat.
You only think it's a bold claim because you still don't understand the problem.